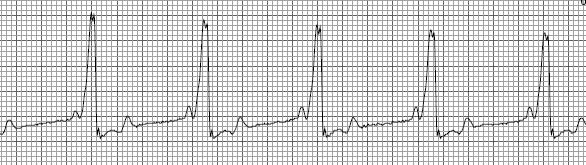
When one compares the complexes and measurements in this EKG, which displays WPW to the Normal Heart Rhythm, you will note four differences. First, the PR interval is shorter than normal, in this example it is .06 seconds vs the normal range of .12-.20 seconds. Second, you will note that the initial portion of the QRS complex does not rise as quickly as normal. This is referred to as a delta wave. Third, the QRS complex is wider than normal, in this case .16 seconds vs. the normal range of .04-.10 seconds. Last, the ST segment is depressed and the T wave is what is called biphasic. The heart rate in this example is 68 beats per minute.
The reason these changes occur is because in addition to the impulse traveling as it normally does through the AV node and the bundle branches, it also travels through an accessory pathway. However, the accessory pathway does not delay the signal (resulting in a short PR interval) and therefore, one of the ventricles is activated prior to other ventricle resulting in the changes described in the above paragraph.
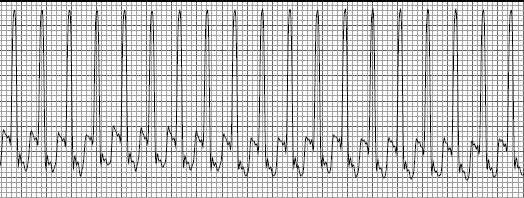
The problem with WPW is not the changes described above, but rather the rapid rhythms that can occur as a result of the accessory pathway. In the normal heart, electrical signals only travel from the atria to the ventricles. However, when an accessory pathway exists, signals can also travel retrogradely, that is from the ventricles to the atria. When this happens, it can cause the atria to become stimulated far sooner than they should since the stimulus is actually coming from the ventricles, not the SA node. This rapid rhythm can then “feed” on itself causing very rapid rates.